Image-Guided Epidural Placement in Parturient Presenting Post-Trauma Spinal Instrumentation
“As an anesthesiologist performing epidurals and spinals, we’re one of the few specialties not using imaging technology regularly to find the epidural space; this is an advancement that is due in our specialty.”
—Stephen Garber MD Anesthesiologist, Medical Director Obstetric Anesthesiology, Saddleback Medical Center
Background
Conventional ultrasound has successfully displaced blind palpation for needle guidance procedures that include central venous access and peripheral nerve blockades. Additionally, the benefits of ultrasound guidance are increasingly clear for assessing and guiding neuraxial anesthesia placement particularly in patients with challenging anatomy.
The efficacy of ultrasound image guidance for neuraxial anesthesia has been proven by over a decade of clinical trials when operated by highly trained expert users. Neuraxial ultrasound has been shown to accurately identify the correct intervertebral level more successfully than manual palpation (1-8). It also accurately predicts the needle insertion depth to the epidural space (9-15), reduces needle insertions and passes, and improves safety (16).
Accuro® is a handheld spinal navigation device that utilizes medical ultrasound to automatically identify spinal landmark anatomy, such as the interlaminar space, in real time. A growing number of clinical studies and trials have demonstrated clinical benefits from Accuro that mirror those demonstrated by conventional ultrasound but with a very low, or non-existent, training burden (17-18). Benefits of neuraxial image guidance are particularly acute in patients with challenging anatomy, which may include a high BMI, patients with previous back surgery, and other presentations where the midline or spinous process is impalpable.
CASE STUDY
A parturient with an ASA Classification of III received anesthesia consult at 25 weeks based on her obstetrician’s recommendation. The patient presented with significant neurological deficits and morbidity secondary to spinal trauma suffered at a young age during a car accident. She had a history of traumatic L1 vertebrae fracture; the postoperative status showed a right L1 laminectomy and fusion of T11-12 to L2-3. Although the instrumentation ended at L 2-3, lateral X-ray demonstrated spaces below L 2-3 were significantly compressed (Figure 1). The patient additionally reported severe chronic pain at the postsurgical scarring and adjacent area and palpation was therefore not practicable. Due to prior surgery and chronic pain, the patient reported significant anxiety concerning ineligibility of epidural placement.
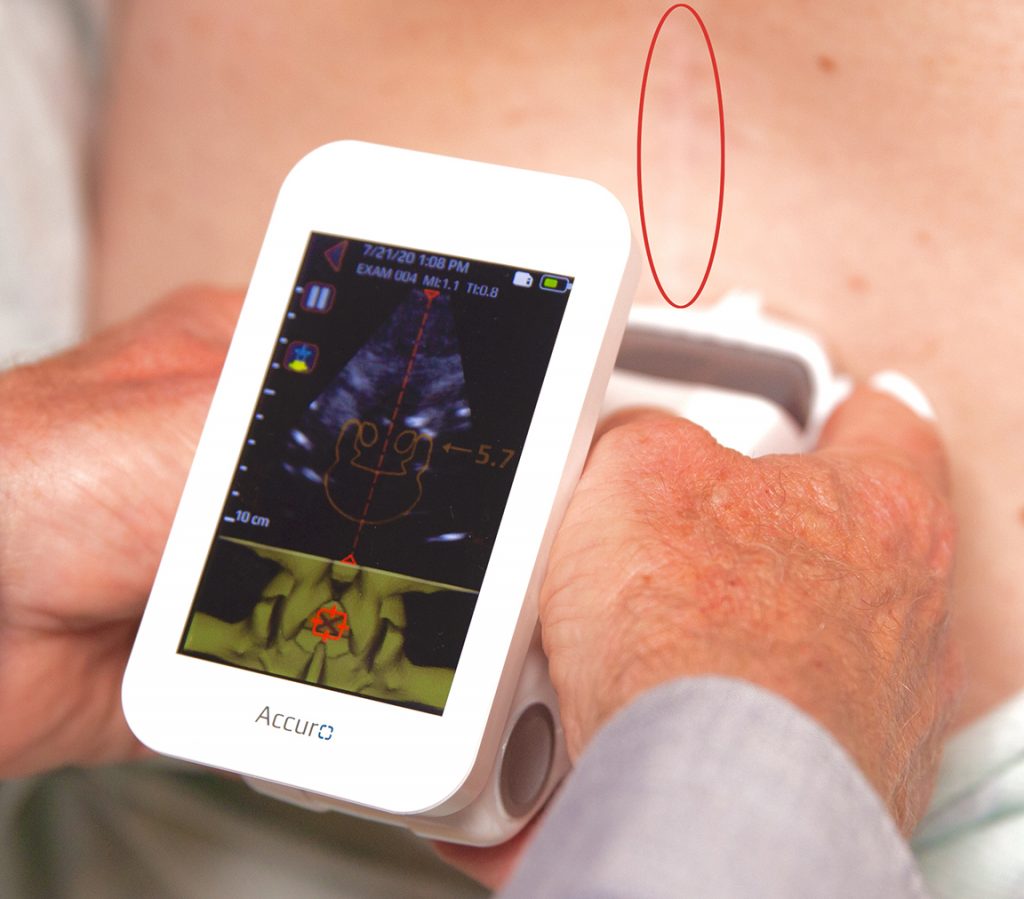
During the consult, the patient’s lumbar spine was evaluated using the Accuro spinal navigation instrument. Based on the Accuro BoneEnhance® image and automated landmark indicators and measurements, an accessible intervertebral level for neuraxial anesthesia placement was successfully identified, presumably at the L3-L4 intervertebral level. Interlaminar space midline was identified by Accuro as substantially adjacent to postsurgical scarring (shown Figure 2). Patient was informed during consult that, based on image guided evaluation from Accuro, successful epidural anesthesia would be possible during labor and delivery.
At 38 weeks, the parturient presented to labor and delivery at Saddleback Medical Center for intended vaginal birth. Consulting obstetric anesthesiologist re-assessed the same intervertebral level using Accuro with equivalent findings to those determined at the 25-week consult. The Accuro Locator needle guide was used to mark the needle insertion site, substantially adjacent to postsurgical scarring, and the automated epidural depth reading reported by Accuro was determined. Neuraxial anesthesia was placed successfully based on the indicated needle insertion site and depth from Accuro. Patient reported low levels of pain throughout remaining labor, and delivered a healthy 7-lbs., 7-oz. newborn.
CONCLUSION
Neuraxial image guidance using Accuro, at both 25-week consult and during labor and delivery, provided essential spinal landmark identification to aid successful neuraxial anesthesia placement in a parturient with postoperative spinal instrumentation and significant compression. The accessible (presumably L3-L4) intervertebral level was identified as a viable intervertebral level compared to other, more compressed or obscured, intervertebral levels with midline adjacent to postsurgical scarring. The implementation of Accuro at the pre-procedural anesthesia consult alleviated patient anxiety and predicted eligibility and placement location for the eventual neuraxial anesthesia placement.
Seasoned Obstetric Anesthesiologists may find Accuro to be effective during and after pre-procedural patient consultation to assess and guide neuraxial anesthesia placement, particularly in patients with challenging anatomy, including difficulties accompanying spinal instrumentation, a high BMI, or scoliosis.
Figure 1. Postoperative X-ray imaging reveals a right L1 laminectomy and fusion of T11-12 to L2-3, with narrowed intervertebral spaces below.
Figure 2. During the 25-week consult, Accuro spinal navigation instrument identifies an accessible (presumably L3-L4) intervertebral level compared to other, more compressed or obscured, intervertebral levels with midline adjacent to postsurgical scarring (red circle).
Resources >
L. Duniec, P. Nowakowski, D. Kosson, T.
Łazowski, Anatomical landmarks based assessment of intravertebral space level
for lumbar puncture is misleading in more than 30%. Anaesthesiol
Intensive Ther 45, 1-6 (2013).
A. J. Lee et al., Ultrasound assessment of
the vertebral level of the intercristal line in pregnancy. Anesth Analg 113,
559-564 (2011).
R. Whitty, M. Moore, A. Macarthur,
Identification of the lumbar interspinous spaces: palpation versus
ultrasound. Anesth Analg 106, 538-540, table of contents
(2008).
H. Schlotterbeck et al., Ultrasonographic
control of the puncture level for lumbar neuraxial block in obstetric anaesthesia. Br
J Anaesth 100, 230-234 (2008).
G. Furness, M. P. Reilly, S. Kuchi, An
evaluation of ultrasound imaging for identification of lumbar intervertebral
level. Anaesthesia 57, (2002).
S. H. Halpern, A. Banerjee, R. Stocche, P.
Glanc, The use of ultrasound for lumbar spinous process identification: A pilot
study. Can J Anaesth 57, 817-822 (2010).
M. J. Watson, S. Evans, J. M. Thorp, Could
ultrasonography be used by an anaesthetist to identify a specified lumbar
interspace before spinal anaesthesia? Br J Anaesth 90, 509-511
(2003).
Daniela Ghisi, Marco Tomasi, Sandra Giannone,
Alessandra Luppi, Lucia Aurini, Letizia Toccaceli, Andrea Benazzo, Stefano
Bonarell “A randomized comparison between Accuro and palpation-guided spinal
anesthesia for obese patients undergoing orthopedic surgery.” Reg
Anesth Pain Med. 2019 Oct; 2019-100538.
K. M. Seligman, C. F. Weiniger, B. Carvalho,
The Accuracy of a Handheld Ultrasound Device for Neuraxial Depth and Landmark
Assessment: A Prospective Cohort Trial. Anesth Analg, (2017).
M. Balki, Y. Lee, S. Halpern, J. C. A.
Carvalho, Ultrasound Imaging of the Lumbar Spine in the Transverse Plane: The
Correlation Between Estimated and Actual Depth to the Epidural Space in Obese
Parturients. Anesthesia and Analgesia 108, 1876‐1881
(2009).
C. Arzola, S. Davies, A. Rofaeel, J. C. A.
Carvalho, Ultrasound using the transverse approach to the lumbar spine provides
reliable landmarks for labor epidurals. Anesthesia and Analgesia 104,
1188-1192 (2007).
T. Grau, R. W. Leipold, R. Conradi, E.
Martin, Ultrasound control for presumed difficult epidural puncture. Acta
Anaesthesiologica Scandinavica 45, 766‐771 (2001).
T. Grau, R. W. Leipold, R. Conradi, E.
Martin, J. Motsch, Ultrasound imaging facilitates localization of the epidural
space during combined spinal and epidural anesthesia. Regional
Anesthesia and Pain Medicine 26, 64-67 (2001).
D. Tran et al., Preinsertion Paramedian
Ultrasound Guidance for Epidural Anesthesia. Anesthesia and Analgesia 109,
661-667 (2009).
M. C. Vallejo, A. L. Phelps, S. Singh, S. L.
Orebaugh, N. Sah, Ultrasound decreases the failed labor epidural rate in
resident trainees. International Journal of Obstetric Anesthesia 19,
373‐378 (2010).
Perlas A, et al. Lumbar Neuraxial Ultrasound
for Spinal and Epidural Anesthesia: A Systematic Review and Meta-Analysis. Reg
Anesth Pain Med. 2016 Mar-Apr;41(2):251-60.
D. Ghisi et al., “A randomized comparison
between Accuro and palpation-guided spinal anesthesia for obese patients
undergoing orthopedic surgery.” Reg Anesth Pain Med. 2019 Oct;
2019-100538.
Singla et al., “Feasibility of spinal
anesthesia placement using automated interpretation of lumbar ultrasound
images: a prospective randomized controlled trial.” J Anesth Clin Res.
2019; 10: 878.
Our website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful. Thank you!
Strictly Necessary Cookies
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
If you disable this cookie, we will not be able to save your preferences. This means that every time you visit this website you will need to enable or disable cookies again.



{kind=link}