
“The future of anesthesia lies in embracing technology to enhance precision, safety, and patient outcomes. Embracing Accuro has not just changed my practice; it has expanded my capabilities as a clinician.”
—Stephen Garber, MD
Background
- Conventional ultrasound has successfully displaced blind palpation for needle guidance procedures that include central venous access and peripheral nerve blockades. Additionally, the benefits of ultrasound guidance are increasingly clear for assessing and guiding neuraxial anesthesia placement, particularly in patients with challenging anatomy.
- The efficacy of ultrasound image guidance for neuraxial anesthesia has been proven by over a decade of clinical trials when operated by highly trained expert users. Neuraxial ultrasound has been shown to accurately identify the correct intervertebral level more successfully than manual palpation (1-8). It also accurately predicts the needle insertion depth to the epidural space (9-15), reduces needle insertions and passes, and improves safety (12, 13, 15, 16).
- Accuro® is a handheld neuraxial anesthesia guidance device that utilizes medical ultrasound to automatically identify spinal landmark anatomy, such as the interlaminar space, in real time. A growing number of clinical studies and trials have demonstrated clinical benefits from Accuro that mirror those demonstrated by conventional ultrasound but with a very low, or non-existent, training burden (8, 17). Benefits of neuraxial image guidance are particularly acute in patients with challenging anatomy, which may include a high BMI, patients with previous back surgery, and other presentations where the midline or spinous process is impalpable.
Case Study
The patient, a 42-year-old gravida 2 para 0, exhibited a medical history notable for advanced maternal age and chronic hypertension, accompanied by severe thoracolumbar scoliosis deemed idiopathic, without concurrent cardiac or pulmonary impairments. Notably, the patient had not undergone any prior therapeutic interventions such as bracing or surgical procedures, and radiographic imaging was unavailable during the case assessment. Conventional palpation methods were impractical in this scenario due to the presence of spinal torsion and curvature, further compounded by the absence of pertinent radiographic data.

Figure 1. Eight weeks prior to the anticipated delivery date, Accuro Neuraxial Guidance instrument identifies an accessible (presumably L3-L4) intervertebral level.
A consultation was conducted with the patient eight weeks prior to the anticipated delivery date to evaluate the potential for epidural catheter insertion. The epidural procedure was accurately confirmed as viable, and the patient was informed during the consult that, based on the image-guided evaluation from Accuro (Figure 1), epidural anesthesia would be possible during labor and delivery.
Admission for labor induction occurred at 39 weeks and four days gestation, primarily prompted by the presence of chronic hypertension. The parturient presented to labor and delivery at Saddleback Medical Center for intended vaginal birth. The consulting obstetric anesthesiologist re-assessed the same intervertebral level using Accuro with equivalent findings to those determined eight weeks prior. (Figure 2). The automated epidural depth reading reported by Accuro was determined, and the Accuro Locator needle guide was used to mark the needle insertion site (Figure 3). Neuraxial anesthesia was placed successfully (Figure 4) based on the indicated needle insertion site and depth from Accuro. The patient labored for 12 hours post-epidural placement and delivered vaginally without incident.
Conclusion
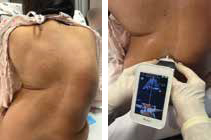
Figure 2. The parturient presented to labor at 39 weeks. The consulting obstetric anesthesiologist re-assessed the same intervertebral level using Accuro with equivalent findings to those determined at the previous consult eight weeks prior.
Neuraxial image guidance facilitated by Accuro utilized both during the initial consultation eight weeks prior to labor induction and during the actual labor and delivery process played a crucial role in accurately identifying spinal landmarks for successful neuraxial anesthesia administration in a parturient presenting with severe thoracolumbar scoliosis. Integration of Accuro facilitated a spinal assessment during the initial consultation, thereby augmenting precision in delineating the epidural space and mitigating uncertainties inherent in palpation-based methodologies. Notably, the Accuro scan conducted during the consultation phase identified an interspace, presumably L3-4, that appeared to be satisfactory for the placement of a labor epidural.
Moreover, the utilization of Accuro technology circumvented the limitations associated with blind palpation as a diagnostic approach, which otherwise might have compromised the inclination toward recommending epidural analgesia. The use of the Accuro during the pre-hospital consult gave some reassurance to both the patient and the practitioner that an epidural placement may be possible.

Figure 3. The Accuro Locator needle guide was used to mark the needle insertion site.
Experienced obstetric anesthesiologists may find Accuro to be a valuable tool both during and following pre-procedural patient consultations, especially in cases involving challenging anatomical considerations such as difficulties associated with spinal instrumentation, high BMI, or scoliosis. The integration of Accuro into clinical practice carries broader implications for academic anesthesia programs, facilitating training of anesthesia providers in the placement of labor epidurals. Accuro enables a level of understanding and precision that may enrich clinical education and enhance procedural outcomes.
References
- L. Duniec, P. Nowakowski, D. Kosson, T. Łazowski, Anatomical landmarks based assessment of intravertebral space level for lumbar puncture is misleading in more than 30%. Anaesthesiol Intensive Ther 45, 1-6 (2013).
- A. J. Lee et al., Ultrasound assessment of the vertebral level of the intercristal line in pregnancy. Anesth Analg 113, 559-564 (2011).
- R. Whitty, M. Moore, A. Macarthur, Identification of the lumbar interspinous spaces: palpation versus ultrasound. Anesth Analg 106,
538- 540, table of contents (2008). -

Figure 4. Neuraxial anesthesia was placed successfully based on the indicated needle insertion site and depth from Accuro.
H. Schlotterbeck et al., Ultrasonographic control of the puncture level for lumbar neuraxial block in obstetric anaesthesia. Br J Anaesth 100, 230-234 (2008).
- G. Furness, M. P. Reilly, S. Kuchi, An evaluation of ultrasound imaging for identification of lumbar intervertebral level. Anaesthesia 57,(2002).
- S. H. Halpern, A. Banerjee, R. Stocche, P. Glanc, The use of ultrasound for lumbar spinous process identification: A pilot study. Can J Anaesth 57, 817-822 (2010).
- M. J. Watson, S. Evans, J. M. Thorp, Could ultrasonography be used by an anaesthetist to identify a specified lumbar interspace before spinal anaesthesia? Br J Anaesth 90, 509-511 (2003).
- Daniela Ghisi, Marco Tomasi, Sandra Giannone, Alessandra Luppi, Lucia Aurini, Letizia Toccaceli, Andrea Benazzo, Stefano Bonarell “A randomized comparison between Accuro and palpation-guided spinal anesthesia for obese patients undergoing orthopedic surgery.” Reg Anesth Pain Med. 2019 Oct; 2019-100538.
- K. M. Seligman, C. F. Weiniger, B. Carvalho, The Accuracy of a Handheld Ultrasound Device for Neuraxial Depth and Landmark Assessment: A Prospective Cohort Trial. Anesth Analg, (2017).
- M. Balki, Y. Lee, S. Halpern, J. C. A. Carvalho, Ultrasound Imaging of the Lumbar Spine in the Transverse Plane: The Correlation Between Estimated and Actual Depth to the Epidural Space in Obese Parturients. Anesthesia and Analgesia 108, 1876‐1881 (2009).
- C. Arzola, S. Davies, A. Rofaeel, J. C. A. Carvalho, Ultrasound using the transverse approach to the lumbar spine provides reliable landmarks for labor epidurals. Anesthesia and Analgesia 104, 1188-1192 (2007).
- T. Grau, R. W. Leipold, R. Conradi, E. Martin, Ultrasound control for presumed difficult epidural puncture. Acta Anaesthesiologica Scandinavica 45, 766‐771 (2001).
- T. Grau, R. W. Leipold, R. Conradi, E. Martin, J. Motsch, Ultrasound imaging facilitates localization of the epidural space during combined spinal and epidural anesthesia. Regional Anesthesia and Pain Medicine 26, 64-67 (2001).
- D. Tran et al., Preinsertion Paramedian Ultrasound Guidance for Epidural Anesthesia. Anesthesia and Analgesia 109, 661-667 (2009).
- M. C. Vallejo, A. L. Phelps, S. Singh, S. L. Orebaugh, N. Sah, Ultrasound decreases the failed labor epidural rate in resident trainees. International Journal of Obstetric Anesthesia 19, 373‐378 (2010).
- K. J. Chin et al., Ultrasound Imaging Facilitates Spinal Anesthesia in Adults with Difficult Surface Anatomic Landmarks. Anesthesiology 115, 94‐101 (2011).
- Singla et al., Feasibility of spinal anesthesia placement using automated interpretation of lumbar ultrasound images: a prospective randomized controlled trial. J Anesth Clin Res. 10: 878 (2019).