Accuro guidance helps eliminate challenges associated with epidural placement for high BMI patients.
By Dr. Regina Fragneto
It’s no secret that childbirth hurts. For most women, it is characterized by intense pain and pressure in the lower abdomen and back – and for some, this can be overwhelming. Many patients choose relief through epidural analgesia, which involves injection of a local anesthetic near nerve roots in the lumbar spinal region. This inhibits nerve conduction, decreasing sensation in the lower half of the body.
But pain relief itself can hurt. Physicians must caution patients that epidural analgesia can lead to complications and some pain may be associated with the epidural procedure itself, adding to anxiety during an already anxious time. These complications can include spinal headache, which can be severe, and soreness at the site of the epidural. While the risk is minimal for the average patient, in certain populations – among them women with high body mass index (BMI) and scoliosis or other spinal deformities – it may be greater due to technical difficulties associated with the epidural delivery. In addition, problematic anesthesia delivery is painful to the medical system due to increased costs of prolonged procedures and patient discomfort and dissatisfaction.
BACKGROUND
Even in today’s advanced healthcare age, epidural delivery can be difficult because many anesthesiologists continue to perform the procedure as if they had virtual blinders on. When attempting to pinpoint the optimal site for injection of a powerful drug, they still rely on their sense of touch to assess spinal anatomy. In obese patients and those with spinal anomalies, needle placement is challenging because physicians cannot successfully palpate the spine to determine the appropriate injection site.
Image guidance for epidural placement would remove the physician’s virtual blindfold to improve accuracy. However, many imaging modalities involve X-ray exposure, which should be avoided in a woman carrying a fetus.
Ultrasound, however, involves no radiation, and research has shown the technology helpful in accurately identifying the appropriate epidural injection site. But performing and interpreting ultrasound requires specialized training and experience that is not in some anesthesiologists’ skill set.
MODERN TECHNOLOGY
Modern technological advances have led to the development of a range of specialized ultrasound devices, including the novel Accuro device by Rivanna Medical (Charlottesville, Virginia). The device applies automated 3D-navigation to spinal ultrasound imaging, eliminating the steep learning curve of interpreting and using ultrasound images to support epidural anesthesia administration. Accuro provides anesthesiologists, regardless of their ultrasound experience, with a clear route to the appropriate epidural site.
Accuro’s image-guidance platform automates measurements of the spinal midline and epidural depth and trajectory in real time. Additionally, the device uses a new bone-specific image reconstruction technology called BoneEnhance. According to a study published recently in Investigative Radiology, Accuro was shown to deliver a five- to 10-fold increase in bone-to-tissue contrast compared to traditional ultrasound.
By contrast to unwieldy, complex, traditional ultrasound technology, Accuro is pocket-sized, portable and battery-powered. It can be carried right to the bedside, making it easy and practical to use in Labor and Delivery, and in a crowded operating room.
At University of Kentucky College of Medicine, we have been using Accuro in Labor and Delivery for about a year. The hospital serves a significant population of obese patients on a busy Labor and Delivery floor. Given that, epidural administration may be uncomfortable and potentially problematic for these patients and a bottleneck for anesthesiologists. In many cases, anesthesiologists are simply unable to palpate a woman’s spine to identify the anatomical landmarks necessary to efficiently perform epidural analgesia.
Without palpation, anesthesiologists have no anatomical information as the basis for epidural placement – and experience, experimentation and guesswork come into play. As a result, the process can sometimes take as long as 30 to 40 minutes, compared to five to 10 minutes for typical patients. During that time, pregnant women sit hunched over and may have to endure several needle sticks until insertion is successful. If the needle hits bone, the result is more pain.
CONCLUSION
Accuro’s automated ultrasound guidance helps eliminate many of the problems of epidural placement for these difficult patients, as illustrated by two cases that I recently observed. In one, a resident and junior anesthesiology attending were attempting to administer an epidural to a C-section patient with a body mass index (BMI) of almost 50, who weighed about 270 pounds. Unable to feel the required spinal landmarks, they struggled for a long time to place the needle blindly. Then the resident suggested using the Accuro. Together they were able to successfully perform epidural anesthesia on the first attempt with the Accuro. This was the first time the attending had used the device and only the second time for the resident.
SECOND CASE
A second case involved a laboring woman with a BMI of 60 who also presented difficulties with spinal palpation. After numerous attempts at blind needle placement, the Accuro was employed to identify the spinal midline and interlaminar space at the correct vertebral level. The epidural catheter was then placed in just a few minutes.
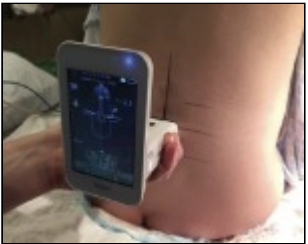
Unlike traditional ultrasound, the Accuro learning curve is minimal. Our physicians simply move the device along the patient’s back to identify the midline and interlaminar space. These landmarks appear as dotted red and orange overlays on the device. In addition, the estimated depths to the spinous process and the epidural space are displayed instantaneously on the Accuro screen. Users mark this location and then proceed with epidural placement. Accuro is so intuitive and friendly that it can be mastered by many within 10 minutes and operated with ease, even with only occasional use.
In addition to Labor and Delivery, a second Accuro device is in use at our hospital by the Acute Pain Service. The device has also been employed occasionally at our institution by pediatric oncologists who encountered difficult lumbar punctures.
Before learning about the Accuro technology, I had been considering purchasing a more traditional ultrasound for Labor and Delivery. However, the use of a traditional ultrasound machine would have been much more cumbersome, as well as being more difficult to use for those anesthesiologists who lacked ultrasound experience. Accuro’s sophisticated algorithms make image-guided epidural placement a reality for our anesthesia team at the University of Kentucky.
“The Accuro learning curve is minimal. Our physicians simply move the device along the patient’s back to identify the midline and interlaminar space […] In addition, the estimated depths to the spinous process and the epidural space are displayed instantaneously on the Accuro screen […] Accuro is so intuitive and friendly that it can be mastered by many within 10 minutes and operated with ease, even with only occasional use.”
 Regina Fragneto, MD
Regina Fragneto, MD
Professor of Anesthesiology
Division Chief of Obstetric Anesthesia
University of Kentucky College of Medicine